



Rosa Escobar and Manuel de Jesús Gonzalez Pineda with their son
Rosa Escobar and Manuel de Jesús Gonzalez Pineda had been together for eight years, though they never formally married.
The two Honduran immigrants living in Nashville planned to remedy that with a ceremony in April. But their plan was put on hold when the coronavirus interrupted church services and other large gatherings. Then, they both contracted COVID-19. Manuel, age 41, fell ill and died, leaving behind his common-law wife and their 4-year-old son Jaison.
“He was a good husband, a good father to my son,” recalls Escobar in Spanish, using a translator. Manuel guided her in Christian faith too, she says.
Gonzalez worked for an excavation company in town. Escobar says she is not aware of anyone from his job or social circles testing positive for the disease, however, so she is unsure how either of them contracted it. When Gonzalez started feeling sick late in March, a clinic did not correctly identify his illness. A few days later his condition had worsened, and an X-ray showed liquid in his lungs.
He was directed to Metro General Hospital, where he stayed until his death two weeks later. After Gonzalez checked into the hospital, Escobar would never see her partner alive again.
Escobar says she had some trouble getting information about Gonzalez’s condition in part because they were not legally married. She faced even more trouble finding someone who could speak her primary language, Spanish — either at Metro General to discuss her partner’s condition, or in her own interactions with Metro personnel when she tested positive herself. The only time she spoke in Spanish with anyone, she says, is when someone at the hospital called to tell her Manuel had died.
It’s an issue that public health officials and medical providers acknowledge and are seeking to address. After Metro identified a cluster of cases around Antioch, where a disproportionate number of immigrants live, the city said it would team with the Tennessee Immigrant and Refugee Rights Coalition to hire community outreach workers tasked with bridging a communications gap exacerbated by the pandemic.
The state has also identified clusters of cases within ethnic groups, and according to health commissioner Lisa Piercey, is working “in very culturally sensitive ways to mitigate any of the issues they may be having.” State health authorities have set up a health disparity task force that is launching a public-service campaign this week targeted at different minority communities around the state.
But it’s not just government agencies spreading information about the disease and related resources to communities where English is not the primary language. Veronica Salcedo’s online Spanish-language news broadcasts offer translations of elected officials’ press conferences (Nashville has a separate Spanish-language briefing) and share public health and other information with Nashville’s Spanish speakers. Her site, Nashville Noticias, was also the first to report on Gonzalez’s death.
Some of Salcedo’s viewers have expressed hesitance to seek out the city’s free COVID-19 tests due to fears that personnel might ask for immigration documentation. Like Metro officials, Salcedo has sought to make clear that the Metro testing sites do not demand immigration information, and she thinks it’s making a difference — more of her viewers are asking how and where to get tested.
Part of the problem identified by Salcedo and others is that many immigrants work frontline jobs that have not shut down, including in construction and at meatpacking plants like the Tyson facility in Goodlettsville, where at least 120 coronavirus cases have been identified.
“We’ve always played this educational and informational role in the community,” says Salcedo, speaking in Spanish and using a translator. “But it certainly heightens during this crisis, as the needs of the community are greater, and the kind of information that they need to receive is greater.”
For smaller immigrant and refugee communities, the challenge can be greater, without local news in their primary language or formalized community leaders. One of Nashville’s fastest-growing immigrant populations is made up largely of Congolese refugees. Kagiraneza Nkuyinka, himself a refugee who moved to Nashville in 2012, has taken on an informal leadership role.
Nkuyinka is an accountant who previously worked with refugees seeking health care, and he also worked for the U.S. embassy in his home country. Earlier this month, he convened representatives from apartment complexes with Congolese residents on a telephone call to disseminate information about coronavirus and related precautions.
He says some Congolese residents have not sought testing because they can’t miss work, as Metro sites are open only on weekdays. He’s also heard fear from those continuing to work in what they consider dangerous conditions.
“My people, with little alternatives, they’re stuck in these jobs they have right now,” Nkuyinka says. “There has to be someone to push, a watchdog who is there to remind people that these people are here, [and] they also need some attention and some consideration.”

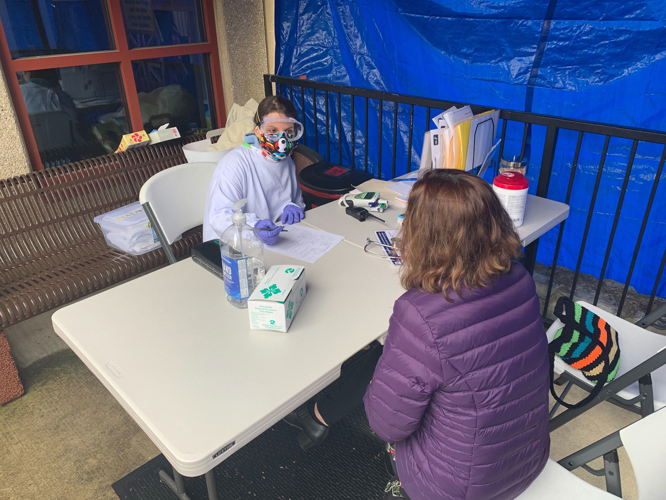
A case worker helps a patient at Siloam Health
One potential salve for the issue is the work of organizations like Siloam Health, a nonprofit health clinic serving the uninsured. According to organization leaders, 95 percent of their patients are born outside the United States, and 80 percent of patients do not speak English.
The clinic set up a “side clinic” in a covered and enclosed space outside its building and has seen at least 16 patients who later tested positive for COVID-19. (Siloam medical director Jim Henderson acknowledges that seeing patients in the partially outdoor space would be more difficult without the moderate temperatures of the past few weeks, and so the organization is talking to contractors about building a more permanent space.) Using interpreters when necessary, providers at the clinic either refer patients to a hospital or send them home with “very strict instructions” about what to watch for, Henderson says.
Offering care and COVID-19 education in a patient’s primary language has obvious benefits for the patient, but Siloam also identifies downstream effects. Once a patient leaves the clinic, they become “useful spokespeople in their communities to spread accurate information,” Henderson says. Even before the pandemic descended on the Nashville area, that was part of Siloam’s mission.
According to Siloam chief community health officer Amy Richardson, community health workers like those employed by Siloam can serve as a “fire break” against disease spread and other health inequities.
“This is a moment in our health care system in the United States that I hope we choose to capitalize on,” Richardson says. “Community health workers really are the front line. They have the trust of the communities they come from and are reaching out to.”



